Poz1956
-
Posts
233 -
Joined
-
Last visited
Content Type
Profiles
Forums
Blogs
Events
Gallery
Everything posted by Poz1956
-
Should I Still Have Sex While On Pep
Poz1956 replied to freshxtop5's topic in HIV Risk & Risk Reduction
PEP isn't always three meds. I've read through 6 different PEP guidelines. With some, depeinding on the doctor's risk assessment, they do have the option of two drug PEP. But yes, logically spreaking bottoming at a sex party would classify as high enough risk for a three drug regime. Fresh: Since you know know the Poz guy was on meds, there isn't much of an issue. Next time you go see the doc, ask him why he only used Truvada. About the side effects. They tend to subside after about a week. Get some generic Imodium and liquid tummy trouble reliever (Pepto, Maylox, Divol etc.) About 50% of people don't finish PEP because they won't put up with the side effects. I like to put it this way, how will you survive the rest of your life on three antiretrovirals, if you become Poz, because you couldn't man up and handle four weeks on a two drug "cocktail," -
I'm not sure if The Sero Project can do more for you than Lamda, but it's worth contacting them. From Sero Project brochure
-
Oraquick Home Hiv Test Window
Poz1956 replied to Internal Blast's topic in HIV Risk & Risk Reduction
With OraQuick the earliest is 4-5 weeks. With lab Antibody/Antigen tests earliest is about 3 weeks. About 90% of people wil have enough antibodies by 6 weeks to show on all tests. By 3 months 99% of people who could show up Poz will be caught. It's very very rare these days for anyone take longer than that. -
Why can't I stop barebacking?
Poz1956 replied to Usedbottom's topic in Making The Decision To Bareback
[sarcasm mode ON] Gee I didn't know that PrEP was only for serodicordant couples! [sarcasm mode OFF] PrEP is for anybody who considers themselves to be a sustancial risk of catching HIV. It is an intellegent pre-emptive move to protect yourself. And like Jizz said - None of your friend's business! -
Undetectabe in Canada is below 40. I left Ontario 33 years ago, so I'm out of touch. Do they have a provincial drug plan like Quebec's? Do you have supplemental medical benefits through work? If so, it's worth checking to see if they will cover PrEP. I've seen deductables in Canada range from zero to $200 (ie I think he said 80% covered, but I need to check with him on that) Personally I've always felt that if a guy was going to lie about anything, he'd lie about his status. He's already given you the one piece of information that is most likely to make you reject him, so why would he lie about anthing sexual health related after that. One guy on here proved me wrong, because he doesn't mention to people that he's not on antiretrovirals If you feel you need some assurance, here's a list of questions you can ask. They are very parallel to the ones you should be asking a "Think's he's Neg" guy. But do it gently and politely. Explain that you're just trying to wrap your head around comdomless sex, and an undetectable viral load. Hell, you can even blame me for suggesting you ask them. When was you last viral load test? How often do you tested? (Probably every 4 months) How many years have you been on meds? How long have you been undetectable? (The standard reccomendation is at least six month, but it sounds like he has probably been UD for years) Have you ever had any blips? If yes, How high did the VL go? Was it back to undetectable at the next test? It's also worth asking when he was last checked for other STIs, In a "if you use it, test it" frame of mind, which orifices? (He's probably vaccinated against Hepatitis A & B. Hep C & Syphilis are probably part of his regular blood work. So that really only leaves Gonorrhea and Chlamydiae as things people routinely test for.) Fisters are at higher risk for Hep C, so that's something you need to get cheked too. A pretty standard rule of thumb is that the longer he's been stable at undetectable, the more likely he is to be undetectable today. A french study said that the lengh of time also increases the odds that his viral load is really and truly zero. Shorter than two years nudged it to possibly between one and 20 As others have said, this is a decision you must make for yourself. It's all about your comfort level. I've got a ton of links I could send you that show the risk is small. I've been accused of Poz busterism propaganda if I just email the info without it being requested. PM me if you want the stuff and I'll send it to you. For example, one item is dated June and from the Quebec Ministry of Health and Social Services. It asked their Committee on Sexually Transmitted Diseases and Blood Born Infections for reccomendations, that will be used to update the province's sexual health guidelines. After reviewing the research, the committee responded with basically the 2008 Swiss Statement, and extended it to include gay couples. Of course, just like the Swiss Statement, it limited the advice to serodiscordant couples. Their rational was that a partner would know if the Pozzie was taking their meds, getting blood work drawn, and attending the routine medical follow-up. (Apparently all the good undetectables are in a relationship, and us bad single undetectables are infectious as hell. I'm not sure how my relationship status impacts my ability to transmit the virus. It all comes back to the standard BS we always hear - You can never trust that a Poz guy is telling you the truth!)
- 13 replies
-
- 1
-

-
- bareback
- undetectable
- (and 1 more)
-
On another forum somebody pointed out something else that make the AHF's propaganda even more misleading. The two right hand bars in thier chart are for vaginal gells containing tenofovir and entricitabine. Technically they are also a form of HIV PrEP. I don't think you can directly compair a vaginal gel, or tenofovir infused cervical ring, with daily oral Truvada for PrEP They are completely different in how they work. The pills are protecting you system wide, while the action of the gells and ring are more localized. Yet one more example of the lengths the AIDS Healthcare Foundation will go, to further their twisted agenda. Though interestingly I did see a quote from Weinstein that said they actually were planning on running a similar ad about the effectiveness of condoms. (I'll believe that when I see it in print, framed with the same negative connotations.)
-
There are so many posts in this thread that say "Assume everyone is Poz!" Frankly that's kind of a bone headed idea, with not much logical thought behind it. For a moment, lets disregard the fact that I've been on meds, and have had an undetectable viral load since the fall on 1999, with never a single blip. Let's pretent I've never taken antiretrovirals. I'm a Poz guy. Should I assume everyone else is Poz? Say they don't choose to have a complete sexual health discussion. Should I just assume they have the same status as mine? Can I just load up thier ass with Poz cum of whatever massive viral load I happen to have at that moment? Unless you had a good discusson around testing, shouldn't the assumpiont be "Everyone has the opposite HIV status to mine!" Arguably, "When," and "How often" are the most important questions. Answers to them give you guidance on how likely the response to "Results" is an accerate reflection of his status today. Of course with the Window Period, even frequent testing and recent results aren't guarenteed.
-
The modern 4th generation Antibody/P24 Antigen lab blood test can pick up a Poz result starting at about three weeks after exposure. More than 95% of people are producing sufficient antibodies to test Poz by four weeks. The standard Western Blot confirmatory test is netorious for taking about 5-6 weeks to register. If you really think you're experiencing suro-conversion illness the doctor or clinic can order NAAT RNA testing which looks for the actual virus, rather than antibodies or angigen. It can detect the virus at about 10-12 days. There is no need to wait for three months to get tested. Since you think you are experiencing the fuck flu, (if it acually is HIV), there is probably enough immyne response to be found by the antibody/antigen test. Rather than wait and worry go get tested NOW. Better for your own health. Better for the health of they guys you play with. Better for your broader gay community.
-
Well if you have any questions, I'd be more than willing to start an online or voice chat, via whatever medium works for you. I think my depth of knowledge could probably handle whatever "interestsing" direction you wanted to take it in.
-
I suspect there's a few of us long time survivors on here who could answer any questions you might have (probably better than most of the doctors teaching you). Or were you asking if we have any questions that we'd like you to bring up in class?
-
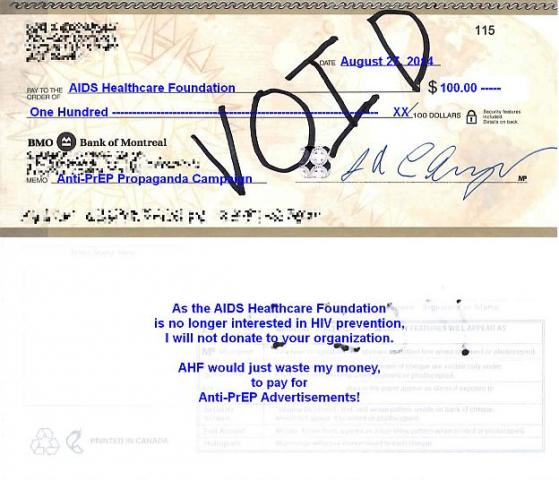
Positive Lite ran an article on this titled "The Truvada Wars: AHF Launches Misinformation Campaign on PrEP." It makes a pretty powerful point. Don't compare PrEP to Birth Control Pills. Compare poor adhearance to PrEP to poor adhearance with Condoms! Would AHF run adverts recommending against condoms, because when rubbers are not used as directed, they Don't Work? AHF is PAYING for these ads to run in print magazines in Florida and California. I find it difficult to understand why the rest of the board of directors is allowing it. This is anti-PrEP propaganda, spewing FUD! (Fear, Uncertainty and Doubt) When I first heard about PrEP, I wasn't comfortable with it. I immediately thought of all the standard arguments against it (without having read them). But after I let it sink in a bit, I recognized it was just another screwdriver in the toolbox. One more thing we can use to prevent the spread of HIV, and a pretty darn good one at that. Why hasn't AHF come to the same conclusion? Maybe it's time for people to vote with their wallets, and stop donating to AHF. How much money have they taken away from AHF's other helpful and constructive initiatives, to pay for all thier anti-PrEP garbage? Ohhhhhh! I just got a great idea of how to make the point. Send them a cheque for some amount (say $100), but write VOID across the face. Add a note on the back saying "As AHF no longer is interested in HIV prevention, I will not donate to your organization. AHF would just waste my money by paying for anti-PrEP advertisements!" (Or something similar) Online outrage is just noise! I understand that politicians consider a letter by postal mail, as worth ten times that of an email. This acts as both a letter, and a financial disincentive. If AHF received enough of voided cheques flooding in through the mail, it would make a very powerful statement! How can we make this idea go viral? Mail to: AIDS Healthcare Foundation 6255 W. Sunset Blvd 21st Floor Los Angeles, CA 90028

-
At the moment there is only one combination approved for PrEP. Truvada which is two NRTI drugs once a day. PEP guidelines differ from place to place. I've read them for five different jurisdictions. Drug and dossage reccomendations are not consistant among any of them. There is leeway for prescribing physician to make choices about the level of exposure risk, and how hard to hit the bug. At the bottom end of the scale is a two NRTI dug, once a day regime. Truvada would be a prime candidate for that. In the middle would the three drug once a day (same as a Pozzie), or two NNRTI twice a day. At the top end of the "Hit it Hard" school of thought, I've seen a four drug reccomendation (2 NRTI & 2 Protease Inhibitor), with three of them taken twice daily.
-
I just tested negative for HIV, but now what?
Poz1956 replied to hungry_hole's topic in What's It Like To Be Poz?
A few weeks before his appointment, Dr. Demetre Daskalakis, the new head of New Your City's Bureau of HIV/AIDS Prevention and Control, said that Doctors who refuse to perscribe PrEP are committing malpractice. That's a pretty strong statement. Might be something worth quoting if you run into a physician who is resistant to prescribing PrEP. -
How many "neg+PrEP" liars do you think are there out there?
Poz1956 replied to rawfuckr's topic in PrEP Discussion
That's a pretty uninformed statment. -
PEP effectiveness is in the high 90s percent wise. While being exposed doesn't necessairly mean you caught the bug, it would still be a wise move. If the exxposure was from an Undetectable Pozzie, you probably don't need to go through the hasstle of PEP. Docs may ask if you know how to contact the guy you think might have exposed you, so they can test him, and/or get his medical data. In some places that contact info has been used to charge the guy, so keep that in mind. The side effects, and how severe they are depends on what drugs are used. PEP guidelines differ from place to place. Some use a two drug regime, others three. As BearBandit likes to say, side effects are not compulsory. If you do experience them, they could include diarrhea, upset stomach, headaches, and/or fatigue. Get a box of generic Imodium (Loperamide) from WalMart or Costco, and maybe your favorite liquid relief for tummy trouble (Pepto, Malox, Divol . . .) Dificulties are worse at the beginning, and will taper off with time. A lot of people wimp out, and don't complete the course of PEP. To be blunt, these are the same drugs Poz people take every day, for the rest of our lives. If we can do it, you should be able to take it for a full a 28 days.
-
The mouth has a lot of defences against getting any kind of infections. It doesn't have the delicate mucous membranes like an ass or vagina. Think of all the potentially bad stuff that frequently goes into people's mouths. Especially babies who put anything that will fit into their mouth, and suck on everything else. They are not constantly getting infections by that route, right? Have you ever followed the "10 Second Rule" on some piece of food you dropped? How about the guys who rim? Rimming certainly does have higher risk of other infections, but considering the number of guys who eat ass, there just isn't an extremely high number of people with mouth infections because of it. Saliva is a part of the body's natural defences against infection. It is pretty acidic, and contains enzymes, and antibodies which kill most bugs. Additionally, the saliva has a tendency to disrupt any cells and viruses which may be floating around in it. And lets face it, what ever was in the mouth, doesn't stay there long. It gets swallowed and put into the extremely caustic environment of the stomach. Additionally, remember that the HIV virus is actually quite fragile. ACON in Australia advises that Swallowing is a better choice than Spitting. The theory is that around the gums is the most likely place for oral issues that might allow infection. Most cum shots happen behind the gums. Swallowing puts any active virus, or infected CD4 cells contained in the cum into the extremely caustic environment of the stomach. The case for Spitting is that the back of the throat does contain some of the same cells as the rectal lining. Since the virus can pass by those cells in the rectum, it is theoretically possible that they could also get by the ones in the back of the throat. That's plausible for a big pre-cummer ram fucking a deep throat. Logically there is a significant difference between a load of cum sitting in an ass, and jiz rapidly passing by throat cells on their way to the stomach. Also those same throat cells are continually washed by mucus and saliva, as you swallow a couple of times a minute. While spitting, you roll the cum around in your mouth, giving it more contact with the gums. When all those thoughts are put together, I think swallowing is the better option. As another point of evidence, I'd like to quote a consensus statement signed by 70 Canadian HIV specialists. While published after the Partner study interim report, it only used data from HPTN 052, and what they see in their own practices.
-
Oral sex is the question that never ends. It is the hardest to study, because very few men have sucking cock as their only risk factor. Transmission risk is VERY difficult to study for higher risk activities, like anal and vaginal sex. Oral sex is almost impossible to investigate thoroughly. There have been three studies that seriously looked at the possibility. Two of them had zero transmissions. One study had several. Researcher interviewed both the newly infected guy, and the person who was the source of the virus, two or three times. Under that scrutiny most admitted to other risks. In only one case, both parties consistently agreed over the course of multiple interrogations. Phylogenic analysis proved a genetic match for the virus in both men. So it is more than theoretically possible. There are a few cases where it has been reported. But please, put it in perspective. How many billions of blow jobs happen every day? More than half of the 35 million Poz people are men. Every Poz guy has been sucked many, many times. Over the 33 years of the epidemic, there are only a hand full of documented cases. Most of those people have had oral health care issues. If oral sex was a good means of transmission, wouldn't most of the gay men in large cities be Poz? If you're going to worry about that small of a risk, you sure as hell shouldn't be considering anything discussed on this site. Also, as with every other mode of transmission, you must take viral load into account. Sucking on a newly infected guy with a multi-million viral load presents a much higher risk than blowing a guy on treatment. Even with those high viral loads, catching HIV is a very rare event. I'd be willing to bet that if you could truly investigate all cases of oral sex transmission, most would be from guys in the acute phase of infection, and the blow job artist had oral health care issues. Last week I had to hand hold a guy through HIV testing. He was terrified, and absolutely certain it would come back Poz. He would not have gotten it done, if I hadn't gone with him. Happily it came out Neg. In the post test counselling, the STI clinic nurse said that oral sex was so low risk, that he should not worry about it.
-
It's important to point out that Danny's math requires that ALL of those tops have high viral loads. In fact, the bottom is Exposed to HIV on each of those occasions. Whether he actually contracts HIV is still down to the correct mix of biological factors all lining up together on any of those fucks. The same article goes on to point out how the extremely high viral loads of an acute infection (someone who caught HIV in the last few weeks but still thinks he's "clean") increases the risk. With viral loads in the one million to ten million range, the risk rises to 1 in 5 exposures. The higher the viral load, the higher the risk. I'm not arguing anything about cumulative risk. It's a given that if he is exposed to high viral load cum often enough, it becomes extremely likely that the bottom will become Poz. It really comes down to luck, and that particular guy's own biology. There are lots of guys who made it out of the 80's and were exposed more that 71 times, but managed to stay Neg. Estimated risks are just a best guess. Regardless of the mathematical calculation of cumulative risk, it is still a roll of the die for each and every fuck. They can help us decide the level of risk we are comfortable with, but they are far from a true predictions of what will actually happen. One part of the original poster's question asked about how many Undetectable Poz loads, and I missed that. Again, given the right biological factors, one fuck could be enough, for a guy who is genetically more susceptible to HIV. We don't know the real chances yet, because there are so few cases in the scientific literature. The Partner study hasn't shown any transmissions from the Undetectable Pozzies in the first two years of the project. We'll have a better idea when Partner2 reports in 2017. Because all the participants in Partner have a previous history of condomless sex, without the Neg spouse becoming Poz, that automatically filters out relationships where the Neg partner is genetically more likely to catch HIV. They call it "The Healthy Survivor Effect." Since the Opposites Attract study is enrolling couples at any stage of their relationship, we expect that some of them will have just gotten together recently. It is possible we could see transmissions occurring in that study due to biological susceptibility. If none of the Neg partners catch HIV in that study we'll have a very good understanding about how low is the risk posed by an Undetectable Pozzie. The final analysis from Opposites, is also expected in 2017. Until both of those studies publish their results in 2017, we'll have to accept the anecdotal evidence that Undetectable Pozzies are unlikely to pass on HIV. If it was happening, we would have heard about it by now. The fact that Treatment as Prevention (TasP) is being heavily promoted by epidemiologists is pretty darn good evidence that transmissions are not occurring very often.
-
Lower_bucks_bottom: The sentence in yellow is a hyperlink to the reference material containing those numbers. The Fall 2012 article titled "Putting a number on it: The risk from an exposure to HIV" is from CATIE (Canadian AIDS Treatment Information Exchange). Footnotes to that piece list the scientific studies from which these numbers are drawn.
-
Questions like this are the exact reason HIV educators are reluctant to give the actual risk statistics. I'll give the numbers, but first I need you to understand what they mean. The chances are exactly like when you roll a pair of dice. Each and every time you toss the die, you have exactly the same chance of it coming up snake eyes. It could be the first time you roll them, or you might never have it happen. The chance of snake eyes has no relationship to what happened on previous rolls. It in no way impacts what number will come up in the future. It takes one fuck from one guy to become Poz. Top or bottom, it's still just one fuck. Be in the wrong place, at the wrong time, with the wrong guy, and it's one fuck. About 83% of new infections are from guys who do not know they are Poz. They all think they're "clean." There are also a pile of variables that we can't predict. Some people are genetically more receptive to HIV. How rough of a fuck? Did it draw blood? Was lube used? The high multi-million viral loads of a newly infected guy greatly increase the chance - and he can't even test Poz yet. The moderately high viral loads of a chronically infected guy who isn't on treatment still pose a relatively "high" risk. But even the continuum from "High Risk" to "Low Risk" used by our HIV educators, is considered "Low Risk" to "Negligible Risk" by HIV specialists. Studies and research show that it is extremely unlikely an Undetectable Pozzie to transmit the virus. We know it is theoretically possible for it to happen if all the wrong conditions existed, but that would be an exceeding rare event. It is very difficult to calculate the risk per exposure. The numbers below are the current best estimates. They are for transmission from a chronically infected individual with a viral load in the 30,000 to 120,000 range. For a bottom the risk is 1 in 71 exposures to the virus. For an uncut top it is 1 in 161. For a cut top it is 1 in 909. Again - that DOES NOT mean a bottom can get fucked by a Pozzie 70 times without catching the virus. Each and every exposure carries that same 1 in 71 chance. It might happen on the first roll in the hay, or it might never happen.
-
Wanting to be a cumslut, but too nervous.
Poz1956 replied to jacobcumdump's topic in Making The Decision To Bareback
About 54% of new infections are from guys who have an acute HIV infections with viral loads in the millions (sometimes 10 million). They caught it sometime in the last few months, but don't know they are Poz yet. Another 30% are from guys who have been Poz for 6 months or more (chronic infection), with viral loads in the 30,000 to 120,000 range. They all think they're Neg, because they haven't been tested in that time. Add that up and you'll see that at least 84% of new infections are caught from guys who don't know they are Poz. Half of guys who have EVER been tested, have not re-checked their status in over a year. The numbers are even higher with guys under 25. It's a myth that you'll catch HIV from the men who know they are Poz. Look up the concept of Treatment as Prevention! -
Wanting to be a cumslut, but too nervous.
Poz1956 replied to jacobcumdump's topic in Making The Decision To Bareback
I'd like to know where the rip in dimensional space/time is located. Can somebody direct me to it? I want to cross over into the parallel universe where some of the guys on here live. The one where being Poz is better than being Neg. The one where being Poz gets you more sex. In my experience being Poz gets you LESS sex. Around 50% of guys agree with the statement "I will never knowingly sleep with a Poz guy." (Backed up by surveys in multiple countries on several continents) Another 20-30% won't agree with "never," but put conditions on it like "only if I loved the guy, or really trusted him." To be blunt, most Neg guys get really nasty, rude, and RUN as soon as they find out you're Poz. They pretend to want the truth, but punish anyone who gives them exactly what they asked for. I think you need to separate the fantasy from reality. Start this way - Name 5 things that will be better because you're Poz. Are any of them not equally achievable by being on PrEP? As a guy who's been Poz for more than half my life, I can tell you there are a fuck of a lot of unintended consequences that you haven't thought of. Like telling every doctor you see from now on. It complicates all other medial procedures. The way some rejections really hurt. Gossip and Stigma. Not disclosing just so you can "get some" is really stressful. How damaging to your self image "Clean," "D & D Free" or any of the other "not me" language gets, after reading it thousands of times. The early aging effects, like serious erectile dysfunction in your 50's, and the way ED drugs don't play well with some antiretrovirals. Trust me - In real life being Poz isn't anything like the fantasies you've read or imagined. -
A doctor does not need to specialize in HIV to prescribe PrEP. You don't have HIV, so why would she need to know all about HIV? Does she need to specialize in HIV to advise you to use a condom? PrEP is just another HIV PREVENTION technique. All she needs to know is how to read some standard blood tests. At the top of the PrEP thread is a sticky with the handouts from Gilead. Print them out and take them with you. (Don't print the big one) Remember YOU are the customer. She is there to serve you. You drive the conversation.
-
The stats for the risk are 1 in 909 if you're cut and 1 in 161 if you're uncut. That's for fucking a guy with a chronic HIV infection with a viral load in the 30,000 to 120,000 range. The chances are higher with a newly infect guy (first few months), because his viral load is frequently in the 1,000,000 to 10,000,000. If you are really scared about it, I think you're still in the 72 hour time frame where you could go to an emergency room, explain the situation, and request PEP (Post Exposure Prophylaxis). PEP is a 28 day course of antiretrovirals that can keep you from becoming Poz even if you were exposed. It's extremely effective at preventing suroconversion. If you want to go on PEP, act now! Don't wait! If it's past 72 hrs since the possible exposure, doctor's won't authorize PEP. Antiretrovirals are the same drugs Poz guys take, and they are also used in PrEP. Speaking of PrEP, if you're going to play BB, maybe you should consider it. US insurance providers cover it, and Gilead has a program to cover the co-pays.
-
While looking for a different video discussion of PrEP, I ran across this one. to PrEP. Considering laws and attitudes in Al Jazeera's home base, I was very surprised to see this well balanced, but mostly pro PrEP piece.