rawTOP
-
Posts
6,112 -
Joined
-
Last visited
-
Days Won
5
Content Type
Profiles
Forums
Blogs
Events
Gallery
Everything posted by rawTOP
-
Given the risk of STIs when we fuck raw, and the fact that there are already drug-resistant strains of common STIs - we'd be kinda fucked if one of those strains to become common. (One of the reasons why I've banned STD fetish on this site.) Were that to happen, getting gonorrhea or chlamydia could require hospitalization. There are 20 million STI infections in the US each year - so this is a BIG problem. And given how poorly a Democratic-led administration is handling Monkeypox, if a Republican is in the White House even less will probably be done since they'll see it as "the wages of sin". BUT THERE'S GOOD NEWS! Rockefeller University is this weird little university here in Manhattan - squeezed into a campus along the East River. No one talks about it all that much, but I keep seeing their name pop up in relation to scientific advances - so they're doing something right… Put into easier terms - antibiotics come from bacteria (since bacteria fight each other). But many bacteria can't be grown in the lab which severely limits the antibiotics that can be studied and deployed. Rockefeller scientists figured out how to create synthetic versions of the bacteria so we can study and deploy a much wider range of antibiotics. They seem to already have one that works on some rather nasty bugs, but many more could from the process they've come up with. Here's the full article with more detail… https://apple.news/Aud-NfBU3R7Sh1kOugUiOfw
-

Justice Thomas makes it clear decisions support our rights are next
rawTOP replied to drscorpio's topic in LGBT Politics
Haven't looked at the bill but I wish it included the right to interracial marriage as well as gay marriage. That way all the Republicans could vote against Clarence Thomas' marriage. Both have the same foundation legally, so including interracial marriage in the bill would make sense. -
I pulled out my childhood vaccination records. There were a total of four shots for Smallpox (18 months, then at 5, 10, 15 years old). I got my first one and then they stopped Smallpox vaccinations. So with only 1 of 4, I assume that gives me zero protection. Backing it up, you'd need to be over 70 to have gotten all of the shots and possibly have some protection.
-
One of my best friends (a fellow New Yorker) is currently standing in line in Toronto to get the shot. He flew up there specifically to get it. Mind you, during COVID Canadians were coming to NY to get shots. Both were ridiculous, bad situations. It's just weird to have the shoe on the other foot. So, here's one of the ethical issues… Should guys refuse the 2nd shot until everyone's had their first shot? I'm thinking yes based on this article… https://www.science.org/content/article/there-s-shortage-monkeypox-vaccine-could-one-dose-instead-two-suffice Barvarian Nordic the company that makes the vaccine. If they say the science behind their product says it's not necessary, I personally think guys should refuse the 2nd shot until everyone's had their first. You can get the 2nd shot any time in the next two years and have the same level of protection as getting it 4 weeks after the first shot. The problem is the CDC disagrees. But do they really know the product better than the CEO of the company that makes it? Canada is only giving one shot (for now). They also pushed "mix-and-match" with COVID and that turned out to be a better strategy than 2 of the same type. I hate to say it, but I trust Canada more than the US right now. They just seem to have their shit together and are making practical, science-based decisions.
-
Yeah, appointments for 9,200 doses here in NYC were all filled in just 7 minutes! https://abc7ny.com/amp/nyc-monkeypox-vax4nyc-vaccine-appointments-how-do-you-get/12055361/ It just goes to show that gay men are willing to end this - we just need the vaccine. This whole thing is completely avoidable and preventable. The bad news is the additional vaccines they ordered won't get here until NEXT YEAR! (See the next to last paragraph in this article…) https://www.medscape.com/viewarticle/977330 Like, what's the point of vaccinating people months after they've caught it? I hate to say it, but I share your pessimism. I think they don't really care 'cause it's "just gay men" and we're sluts. It certainly looks like the Biden administration is counting on herd immunity through inevitable spread. The fact that it's avoidable and takes 2 to 4 weeks out of our lives isn't really a big deal to them. As long as people aren't dying they don't seem to really care. The sad truth is there's not much we can do about it. Not voting or voting for Republicans will only make things worse. All we can do is vote for whoever challenges Biden in the primary. And it's not like it couldn't be different. They seem to have all the vaccine they need in Canada. I just walked into a vaccine center in Toronto, gave my mother-in-law's address and phone number, and they gave me a shot. No appointment necessary and the line wasn't even all that long.
-
Justice Thomas makes it clear decisions support our rights are next
rawTOP replied to drscorpio's topic in LGBT Politics
You mean like this? -
Even if you bring your own toys - if the top has it there's a good chance you'll get it from him because he's handling your toys. If he touches you, there's risk. If you touch his clothes that have touched his sores, there's risk. It goes on and on… So boot licking might be low risk if that's your only physical contact. Piss will have risk. Sucking cock definitely has risk. I mean if cuddling is risky, pretty much everything is risky. They're talking about not getting bigger quantities of vaccine until this fall or even next year (in the US at least). So the situation is rather dire the next few months. I think it's already spreading pretty quickly among the guys who are most active sexually. Which means there will be a fairly big pool of piggy guys who have natural immunity. Add the fortunate few who can get a vaccine. And then add the piggy guys who are willing to "get it and get it over with" and are willing to give up 2-4 weeks of their life so they can continue being piggy. I think in a couple of months those will be the guys at the parties and clubs (that are still open) while the majority of guys scale way back on things until vaccines are readily available. Not sure about the UK and Canada, but the sex scene in the US won't be back to normal until some time next year, IMHO. In the meantime what parties there are should be a lot of fun since they'll have the piggiest guys who got it (and a few lucky vaccinated guys).
-
This was written by a queer person in Toronto who got Monkeypox. Gives their take on what to do if you get it… https://www.igotmpox.com/
-
Justice Thomas makes it clear decisions support our rights are next
rawTOP replied to drscorpio's topic in LGBT Politics
I predict that we will lose the national recognition of gay marriages within 5 to 10 years. The threat is real unless people stand up to what's going on right now. Justice Thomas isn't fucking around. He has real power and he's using it. Oh - and the porn you like to watch? Good luck with that as well… Notice how the GOP has started labeling everything that's LGBT as "pornographic" (e.g. yesterday's news story). They want to suppress people's freedom of sexual expression on all levels. The Democrats are far from perfect, but the GOP has changed over the past 20-50 years and IMHO they're now the mortal enemy of people like us. I'm just hoping enough moderates (and women generally) will be upset enough about the Dobbs decision that they'll get out and vote Democratic in November. If the tide doesn't turn in November I'm really worried about 2024. -
One is a complete violation of BZ’s rules, the other may or may not be. I take explicit, intentional violations far more seriously. When I reconfigure chat I’ll ban Telegram just on the basis of being in competition with it. But it will be a soft ban with no infractions unless someone tries to circumvent the measures I put in place.
-
In what universe is it acceptable to encourage someone else to do suicidal behaviors? If you can’t figure out that that’s a bad idea you don’t belong on this site. There are no fine lines on this issue. “Never take meds” = suicide = must be discouraged.
-
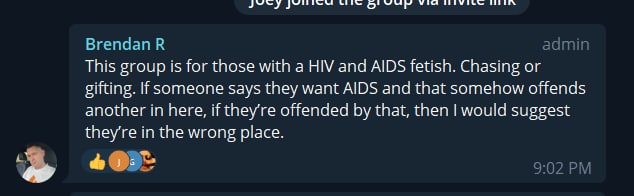
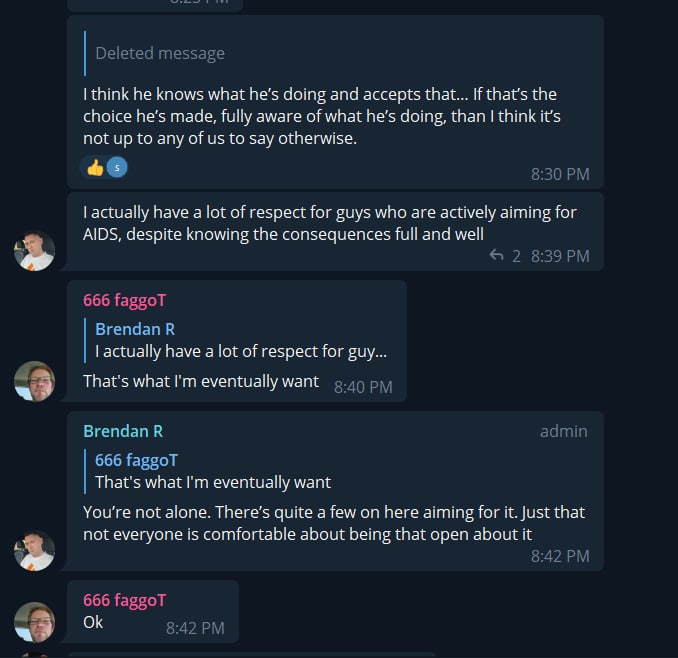
BTW, here is a screenshot of one of the moderators of the Telegram group saying it's an AIDS fetish group and defending the guys who fetishize progressing to AIDS intentionally (and presumably dying). And here's the same moderator talking about how admirable it is to intentionally progress to AIDS. (Remember - that's literally suicidal and promoting that when you're in a position where you can squelch or redirect it, is harmful to the community.) I know I'm being badmouthed by WelshBBCigarFuck on Telegram. But he's talking out of his ass. It clearly is an AIDS fetish group. And I'm guessing it got most of its members by its admins promoting it in posts here on BZ. My enforcing this sites rules shouldn't come as a big shock. My taking away the status of people involved in violating this site's rules shouldn't be shocking either. And me banning a member who flat out lies to me and won't stop arguing with me when he's clearly wrong is pretty normal as well.

-
If anyone is wondering… WelshBBCigarFuck continued to argue with me over the issue so I banned him for a year at which point he requested his account be deleted, which I did. I know for a fact that his representation of the Telegram group wasn't truthful. Someone I trust absolutely told me as much very clearly and showed me screenshots where moderators defended the AIDS fetish aspect of the group. Sorry, but that's suicidal behavior and I won't have this site be used to fetishize suicide. So the moral of the story is that you shouldn't pick and pursue unwinnable fights, and make false statements to the owner of whatever site you're on. It won't end well. But account deletion was his idea, not mine. I just wanted him to stop arguing with me.
-
You have been downgraded because of our discussion about promoting an AIDS fetish Telegram group that you're involved in. Unlike the Telegram group, which permanently bans people for questioning the fetishization of going without meds to the point of getting sick and dying, you're still allowed to use this site. It's just you've been stripped of your status here. Put another way - you're feeling the effects of a policy that's more generous than the one in place at your Telegram group. The same measures was taken with @timfreo who is also involved in the AIDS fetish group and had promoted it widely here before I realized its nature. Bottom line - I'm completely serious about not tolerating AIDS fetish on this site. This site will absolutely not be a vehicle for encouraging suicidal behavior.
-
Meningitis outbreak in S Florida
rawTOP replied to jdubya's topic in HIV/AIDS & Sexual Health Issues
As @ErosWired stated - THIS IS SERIOUS - GUYS ARE DYING!! You can avoid all the risk by getting a simple vaccine. I got mine a number of years ago when NYC had an outbreak. So, GET VACCINATED SOON! Here's an article on it from a highly reputable source (website aimed at doctors, not patients)… https://www.medscape.com/viewarticle/976126 -
Yes, that list was developed before PrEP and is 10 years out of date.
-
If HIV is a gun, then PrEP is a bulletproof vest. And the guy who wants to stay neg, but takes loads from complete strangers without asking their status, yet doesn't take PrEP would be like someone who wanders onto an active shooting range. Where HIV isn't like a gun is that it's less likely to kill. And PrEP is far more effective than a bulletproof vest - so that analogy isn't perfect either. When you have the ability to protect yourself and you refuse to use the protection while simultaneously putting yourself at significant risk - IMHO, the only person who is at fault is the neg guy. Simply put - in scenarios like that YOU are the only one who is responsible for your health. Since PrEP offers very close to 100% protection, I fail to see how the toxic poz guy could be "unethical" for blowing his load up neg asses. He won't actually infect anyone unless they're actively or passively bug chasing. Now, if he's specifically targeting say closeted 18 year olds who are still living at home with parents watching their every move (and hence don't really have access to PrEP) - yeah - that's unethical. But cases like that aren't typical. But if he has some random, anonymous hookup in a park with the same kid - then I don't see that as unethical either. There are now three different types of PrEP, so there isn't even the argument of "well, the neg guy couldn't tolerate Truvada". If you want to stay neg and you're taking loads from strangers / people you don't know all that well - then you need to be on PrEP. If you opt not to take PrEP and you get pozzed - it's because of your action/inaction, not the action of the poz guy. All of that is a little off-topic - except to say I don't see it as unethical to stay off meds and be sexually active. But just like the neg guy should be responsible for his health - the poz guy should be responsible for his health and go on meds when it's time (CD4 <= 500, if not sooner).
-
They aren't to be trusted - especially big pharma. Just one simple example - Descovy should have been available for PrEP YEARS ago - everyone knew it was (more-or-less) the safer version of Truvada. But Gilead let people suffer side effects from Truvada in order to make more profits. They ran with Truvada as long as they could and then got Descovy approved for PrEP just in time so they could extend its patent and keep the cost of the drug high. As far doctors… Here's a little bit of what's happened to me personally… At one point I went to this gay doctor who treated a lot of HIV/AIDS patients. Literally every time I went to see him there was a pharma rep in his waiting room. It was completely obvious he was getting paid to prescribe meds that were the most profitable for the drug companies. Ethical docs don't take meetings with pharma reps - they go to educational / neutral sources to get their information. And from my time in pharma marketing - when a doctor like that is also recognized by his peers the pharma companies groom them to be "thought leaders". Those are the people who present even the "educational" seminars (aka "grand rounds" lectures). It's just in the "educational" sessions they have to use the generic name of the drug, not the brand name, and they have to also discuss other competing drugs (but guess which ones the thought leaders will say are best?) And… I was a 26 year old kid when my lover was in the hospital with AIDS. A doctor had told me he needed his IV drugs in a certain order. When the nurse went to give him the meds one night the order she was giving them in seemed wrong to me. I questioned her and was told in no uncertain terms that she was right and I was wrong. I woke up the next morning (we had a private room in the hospital where I was sleeping with him) to find him in distress. His heart rate was up around 180 and it had been like that for hours. Basically she HAD given the drugs in the wrong order, and he had done the equivalent of running a marathon all night. He never really recovered from that. A few months later he died. And a year later ARVs came out. If he'd been able to survive another year he might still be alive today. I was young and "white coat syndrome" was at play - I didn't make her stop and call a doctor over. But it taught me you can't trust medical professionals. It was probably unintentional - but she basically killed him. Another first-hand case… When I was 18 I was told I had a seizure condition. A couple years later MRIs came out and I was told I had a brain tumor. Years went by and nothing happened and I didn't always see doctors to stay on top of it. Then I started having blackout spells again and a friend got me in to see the head of neurology at Memorial Sloan Kettering who was a brain tumor specialist (MSKCC is one of the top cancer hospitals in the world). She put me on dilantin and ordered a biopsy (which is a pretty high risk surgery) that was done by the Chief of Neurosurgery. The result was "scar tissue" but they continued to believe it was a brain tumor since tumors can be surrounded by scar tissue. Years went by again and when there was another round of blackouts she ordered another biopsy. This time the neurosurgeon was more aggressive, but the result was still scar tissue. 15 years had passed since I was first diagnosed with the tumor. I asked my doc whether the progression they saw could simply be higher MRI resolutions seeing more of the mass. She said no. I told her I wanted to go off dilantin since I was having problems with my gums (a well-known side effect of dilantin). She told me if I wanted to do that I needed to find another doctor. I took myself off dilantin (it has to be done over months), and eventually found myself another doctor. That doctor sent me to a radiologist who thought my case was unusual. He was the first radiologist in all those years who actually sat down and talked with me. I lent him 22 years of scans and he took a half a day to pour over them. His conclusion was that it was just a scar (as the biopsies found) and the apparent "growth" was due to 1) increased MRI sensitivity (I was right), and 2) MSKCC going in and making the situation worse by doing multiple biopsies. As far as my blackout spells - they're just simple vasovagal reactions - not epilepsy. I didn't need dilantin (and it was harming me - my oral health hasn't been the same since). So I've personally witnessed a nurse at one of the top AIDS hospitals do something which essentially killed my lover. And I've experienced malpractice by doctors who are arguably some of the top in their specialty in the world. I now prefer doctors / NPs who graduated from state schools - they're less cocky and arrogant and are more likely to question their own judgement - which in my view is essential in healthcare. So yeah if you think I don't think trust doctors - you're absolutely right. I question everything and only do what makes sense to me. If a doctor is bothered by my questions I find another doctor. I do take their opinion seriously, but I make the final decision. And pharma companies - they're only in it for the money - not for saving lives. It's why there are so many treatments and so few cures.
-
Consequences for taking high viral count loads
rawTOP replied to Daddysapig's topic in HIV Risk & Risk Reduction
It's a good question. Back before ARVs there were no meds-resistant strains because there were no meds. The folk wisdom at the time (not sure if it was based in any science) was that it was good to challenge your immune system with new strains because your immune system gets in an equilibrium with your strain but when presented with a new strain your immune system kicks into high gear, produces more antibodies, which fends off the new strain and helps control your existing strain. My understanding is that you only have one dominant strain of HIV at a time (unless you're a rare case who has both HIV-1 and HIV-2). The existing strain usually wins when challenged by a new strain, but not always. So even back then guys were risking a more aggressive strain winning over an established mild strain. But the reverse could happen as well - a strain with fewer effects, but more "fitness" could win out over a harsher but more fragile strain. But since ARVs came out none of that exactly applies these days. These days the risk for undetectable guys is that they take a load that's meds resistant to the meds they're taking and then their meds stop being effective and then they've got a meds-resistant strain. What I don't now is whether, if that happens multiple times, will it will narrow the number of meds that will work for him? There are a limited number of types of meds and there are some strains that are resistant to a lot of meds - which are clearly bad news if one of those becomes your dominant strain. The more you chase strains the more likely you are to get one of those bad boys. I've known friends-of-friends who've died that way, but I don't know if they had other issues - like drug use, or if they were taking their meds properly, or how damaged their body was when they first started meds (they were typically pretty long-term survivors). So a question for someone who knows more than me… If a toxic guy who had a strain that was meds-resistant for A & B sought out more strains and had another strain that was resistant to C & D take over as his dominant strain, would he still be meds-resistant to A & B from the earlier strain? -
Actually that's not what I said. I said guys should absolutely go on ARVs when their viral load was between 350 and 500. Which means they probably should go on when they're around 500 (if they didn't go on sooner). And I repeatedly mentioned 350 because that was the threshold used by the study. It's not like CD4 counts go in predictable straight lines. So someone might go below 500 because they have a cold or something and then be up over 500 on the next test. But when the trend is clearly below 500 guys should go on meds IMHO. As I understand it that was the standard model of care in most of Europe for a very long time and it works pretty well. It's just START showed that going on meds immediately was marginally better for the individual, and substantially better from an overall public health perspective. I'm so against the idea intentionally progressing to AIDS that I've banned it from the site. I think I've made it pretty clear that I view that particular fetish as literally suicidal. The point with this post is that there's a gray area in between going on immediately and "no meds ever" and it's not an unreasonable option for some guys. As far as your "You will already be at higher risk for…" statement - my point is that the START study was the major study behind statements like that and the conclusion was that "the absolute differences were fairly small". If you have other studies that show otherwise, please share them. With a larger sample size your confidence interval shrinks. When your confidence interval shrinks to the point that there's no overlap in the groups being compared, then the finding is "statistically significant". Ergo, statistical significance is directly related to sample size. In this case yes, 1.4% is > 2x 0.6%. But my point is that both are extremely small. (1.4% wouldn't be small if we were talking about an outcome of death, but we're just talking about "complications".) By focusing on the statistical significance and not the absolute risk being discussed you're not seeing for the forest for the trees. The doubling from 0.6 to 1.4 is important from a general public health perspective, but it's less important from the perspective of an individual. My impetus for posting it in Sexual Health is because the poz fetish crowd deserves sexual health as much as everyone else. Calling them "lunatics" is completely unproductive. I'm seeing a disturbing trend of making these issues black and white - that there are two and only two camps - 1) go on meds immediately or 2) "never take meds". The data says there's a middle ground where you can delay without significantly risking your own health. Guys who choose to wait need to understand the numbers so they know the point where they really need to get themselves on meds (before they have actual complications). The purpose of my post was to present a risk reduction strategy that some guys might choose over intentionally progressing to AIDS. If I can get those guys to move from thinking in terms of "never take meds" to "delay while my CD4 is good" - that's a huge win. Those guys are unlikely to ever switch to "go on meds right away", but "delay for a while" is an achievable goal with that group, IMHO.
-
The bug chasing and gift giving sections on this site are quite popular, so the timing of when poz guys go on meds is directly relevant to a lot of the guys on the site since it's kinda obvious that the longer you stay off meds the more bug chasers you're likely to poz. The main study that people cite when they tell you to go on meds immediately after infection is the START study. You can read the result of the study here: Initiation of Antiretroviral Therapy in Early Asymptomatic HIV Infection That study divided people into 1) start right away, or 2) start when the person's CD4 (t-cell count) was around 350 (which is above 250 where the person would be diagnosed with AIDS). Most medical professionals will tell you that you improve your odds of staying healthy by going on meds as quickly as possible. And that's technically true, but the benefits of going on meds quickly aren't as large as they often imply. The first thing to realize is that the word "significant" in a scientific study has a different meaning than it does in everyday use. Statistical significance is directly related to the sample size used in the study (the number of people being studied). The rule of thumb is that sample sizes of 1,000 or more will result in statistically significant results. The START study had a sample size of 4,685. Because they have a sample size 4x bigger than is needed all of their results are statistically significant. So when you read the results of the study (or read someone talking about the study) you can ignore the word "significant" - in this context it doesn't mean what it means when it's used in everyday conversation. Since all the results are statistically significant, it's literally meaningless. It's like reiterating "…and that was concluded off of a large study". For starters their big measure was whether someone had significant health complications over the study period which was 3 years on average. 42 people in the immediate start had complications, 96 in the delayed start had complications (page 799). So yes, you're a bit more than twice as likely to have complications if you delay the start. BUT 42/2326 = 1.8% over 3 years (so 0.6% per year) vs 96/2359 = 4.1% over 3 years (so 1.4% per year). If it were a matter of doubling a 10% risk, I could see the point. And from a public health perspective I get the point. But from a personal perspective a 1.4% chance of a complication each year isn't that much. They actually say as much… So if you're someone who already has serious health issues that would be complicated by HIV - absolutely go on meds quickly, because every little bit can help you. Or if you want to make sure you don't transmit HIV to anyone else - absolutely go on meds quickly. But apart from issues like that - it's your body, your health - you're allowed to choose not to go on meds right away. Do what makes the most sense in your situation. The other issue with the study was that six of the (numerous) sponsors of the study were pharmaceutical companies. Most of the discussion of this study makes it sound like it's imperative that people start HIV meds immediately. I worked in pharmaceutical marketing in the late 90s. We recruited "thought leaders" who would push other doctors to do what the pharmaceutical companies wanted them to do. The fact that a study that said that "the absolute differences were fairly small" is getting spun to "you must go on meds immediately" - that's doctors saying what the pharma companies want them to say. The pharma companies got their thought leaders to convince other doctors to say that. When it's done well the process is really subtle. I know because that was literally our job (for other drugs/conditions) - the company I worked for published journal articles for pharma companies and organized promotional and non-promotional meetings for them. The non-promotional meetings were often fairly ethical (e.g. getting the word out to busy doctors about a new, effective drug). But in hindsight the promotional meetings and the journal articles (where bad results are never published) were usually really unethical. The promotional meetings were often at ski resorts, or golf clubs. Even the quickie follow-up meetings were at really expensive restaurants. I should also mention that the START study was published in 2015 and there's been more research since then that's pointed to other possible benefits of starting meds early. But the research I'm aware of is mostly about whether people can be completely cured of HIV at some point in the future and those studies have hinted that there's the possibility that having gone on meds quickly will help in that respect - but AFAIK there hasn't been any firm conclusions on that since only about two people have ever been permanently cured of HIV (via a procedure with a 20% fatality rate - they were cancer patients so the risk made sense). And I want to make clear - I'm absolutely opposed to the "never take meds" folks. Yes, you have the right to commit suicide, but I'm never going to encourage someone to do so. And it literally is suicide to not ever take meds, or to take them haphazardly once you need to start them. The medical/scientific community generally agrees that you absolutely should go on them when your CD4 drops into the 350 to 500 range. Please go on at least by that point. A 1.4% per year risk of mostly non-fatal problems isn't crazy. But in the mid-90s (before ARVs came out) I cared for a lover who died of AIDS - it's not pretty and it is literally suicidal to want that experience when there are meds to prevent it. As a bottom line I'll repeat - it's your body - make the informed decision that you're most comfortable with. Your doctor should not make you feel like you're crazy if you want to wait a bit to go on meds (provided your CD4 stays over the 350-500 range).
- 27 replies
-
- 14
-

-

-

-
Not only that, our current Vice-President co-sponsored FOSTA/SESTA. So the situation is unlikely to change any time soon. https://filtermag.org/presidential-hopeful-kamala-harris-made-sex-workers-lives-more-dangerous/
-
"You are only allowed to send 0 messages per day"
rawTOP replied to a topic in Tips, Tricks, Rules & Help
To answer some of the recent questions… What you can do depends on your member rank - the one shown under your avatar when you do a post. When it no longer says "New Members" you'll be able to do things like DMs and ratings. As that continues to change you can do a larger number of DMs and ratings. And the logic of allowing you to do public posts before DMs is pretty simple - spam in public posts is caught and reported more quickly since it's seen by more people. And also the site benefits from public discussion - much less so from DMs. -
"You are only allowed to send 0 messages per day"
rawTOP replied to a topic in Tips, Tricks, Rules & Help
I should add that if I had my way I'd let Senior Members initiate conversations and then have zero limits on those conversations. But the software that powers this site isn't that flexible. And I know I've said I'm developing other sites and it's been forever and you probably don't believe me by now. BUT after a few years where I wasn't making much progress, I'm back at my programming. For personal reasons chat and messaging aren't my top priority right now, but I will get to them in the coming months. Once I do that, the other sites will be better for DMs. (Hopefully I can do it in a way that's not too confusing.) -
For far too long @drscorpio has been doing the bulk of the moderation here. I'm happy to announce that, going forward, @viking8x6 and @a6uldeve84u will also be moderating your posts. a6uldeve84u has been with the site for 11 1/2 years, viking8x6 for 9 1/2 years. Please be kind to them - especially the first few weeks as they learn how to be moderators.
- 19 replies
-
- 29
-
-
-