rawTOP
-
Posts
6,112 -
Joined
-
Last visited
-
Days Won
5
Content Type
Profiles
Forums
Blogs
Events
Gallery
Everything posted by rawTOP
-

Governmental Porn Blocks Have Started – How Circumvent Them
rawTOP replied to rawTOP's topic in LGBT Politics
You've got to be typing in a bad URL. ALL of the following should work… breeding.zone http://breeding.zone https://breeding.zone breedingzone.com http://breedingzone.com https://breedingzone.com www.breedingzone.com http://breedingzone.com https://breedingzone.com In addition there's (http:// | https://)www.breeding.zone which goes to the site where the chat feature runs, but there's a link to the forum on there. If you can tell me exactly what you're doing when it doesn't work, then maybe we can figure out what you're doing wrong. -
Justice Thomas makes it clear decisions support our rights are next
rawTOP replied to drscorpio's topic in LGBT Politics
I think for him it was transactional. He supported a policy he didn't necessarily believe in because it would give him needed support from a large group of people without whom he couldn't win the presidency. And he knew continuing to support their agenda would be his best chance to retain power. -
The Michigan Supreme Court has ruled that discrimination against LGBT+ folks is sex discrimination under Michigan's anti-discrimination law! https://apple.news/A0qJZ3nK1QxyakO7ITaJGVA
-
If this is your source for saying 85% efficacy… That source does not say that a 50 year old, incomplete vaccination is 85% effective. In fact it's unclear what they're talking about. The way I read it they're talking about JYNNEOS and they acknowledge that it's based in part on animal studies, not studies in humans. It's always better to err on the side of caution. Hence my comment that one shouldn't assume protection from 1 or 2 shots 50 years ago.
-
The smallpox vaccination was a series of 4 shots at 18 months, 5-6 years (just before school), 10 years and 15 years. The US stopped giving that vaccination in 1972. As a result you'd need to be over ~65 years old to have had all 4 shots, over ~60 to have had 3, over ~55 to have had two. I wouldn't count on much of any protection unless you had 3-4 shots.
-
Governmental Porn Blocks Have Started – How Circumvent Them
rawTOP replied to rawTOP's topic in LGBT Politics
ALL browsers on iOS are Safari. The only thing Apple allows developers to do is change the user interface of Safari. Actual other browsers are banned from iOS devices. That means Firefox on iOS isn't really Firefox - it's Safari with an interface done by folks at Mozilla. -
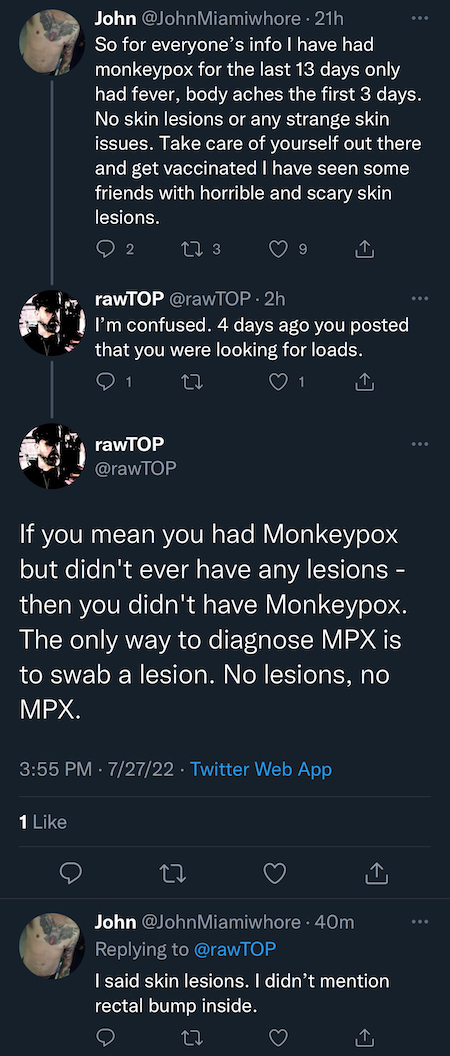
Just had this interaction on Twitter… Can someone please explain to me how the guy's logic makes any sense? He says he's had MPX for 13 days (which is a remarkably short time) He says days 1-3 were body aches and fever (that's believable - but probably not for minor case) That means days 4-13 he was symptomatic (10 days of having lesions). All the health authority websites say the lesions last for at least 14 days - and you're infectious for another week after that while the skin grows back over the site of the lesion. 4 days ago (day 9, 6 days into having lesions) he tweeted "Poz ass here looking for loads tonite". How can you be 6 days into having anal lesions and want to get fucked? Any activity down there would be horribly painful with anal lesions. He seems to be differentiating "skin lesions" from lesions on the skin inside your ass - fine, no problem I get what he's trying to say. But I would think lesions in your ass would take a longer time to heal than lesions on your body since it's a less hygienic location. You're not done and ready to go after 10 days. And there's no mention of getting tested. Given that he's presumably in Florida where testing would be hard to come by, I'm 99% sure he doesn't have a positive test result. Either way, takeaway #1 is that he believed himself to have anal MPX and he was trying to get tops to fuck him while he thought he was infectious. That's disturbing. And if he did have MPX he's still infectious. I'm not sure what he had, but I'm almost certain it wasn't MPX. Last I knew he was poz and not on meds. So it could be his weakened immune system acting up and then causing an anal herpes outbreak (which typically goes away in a week). The problem is now he's gonna think he's got antibodies to MPX. When (not if) he gets the real thing maybe then he'll finally understand what it means to have it. In the meantime he's blocked me.

-
From the sounds of it, the US will start getting a lot more doses this fall and early next year. So 6 months might be enough of a delay, though it might need to be 9 months. Personally I trust 1) the company that makes it, and 2) Canadian health authorities more than I trust US health authorities. The Canadians just made smarter choices when it came to COVID (at least medical decisions - their contracts to actually get the vaccine were seriously flawed).
-
Except people with MPX aren't thought to be infectious until lesions form…
-
Here's another thought… If it's super painful, and especially painful to the touch, then how do guys with MPX transmit it sexually? Wouldn't sex be super painful? OK, maybe the first day or two when the lesions are small they could have sex. But that doesn't explain the huge levels of transmission that we're seeing. I suspect that there are mild cases that are so mild people don't realize they have it. Since you need a lesion to do the test, all those cases wouldn't be reported, which means massive under-reporting. That would explain the high levels of transmission that we're seeing. Until there's something like a blood test that can detect it, I don't think we can get a handle on how many active cases there are.
-
One of my best friends is going through a pretty painful case of MPX at the moment and his husband has managed to not get it despite being in the same house. Mind you they were both vaccinated (probably right after my friend was exposed). So by now the husband's vaccination is helping him avoid it. Point being - it is absolutely possible to be around someone and not catch it - just depends on the nature of your interaction (and probably a little bit of luck).
-
What it's like to have Monkeypox
rawTOP replied to JakeTurner's topic in HIV/AIDS & Sexual Health Issues
Some guys on Twitter are sharing their experiences which seem worse than the ones mentioned here, so I figured I'd include those as well. Click "view" to see the content (since Twitter has them locked down since they're mostly posting porn)… Silver Steele HungerFF Ziven Sparks Ziven wrote out a full blog post with his experience… https://medium.com/@zivensparks/a-sex-workers-monkeypox-experience-5d8b3e4560d6 -
I think the issue is that the best way for MPX to spread is skin to skin contact with a lesion. Group sex is perfect for in that respect. Add on that young, intrepid, more sexually active guys are at higher risk since the didn’t get any smallpox vaccine as a kid… MPX on surfaces is less perfect. There may not be enough virus to cause infection. Or exposure to less virus => less severe infection as we see with COVID. So I think it’ll tear through the gay community and then unpredictably pop up here and there amongst the straights. For us this will be a bit like HIV - either you get it (just once) or you get vaccinated (similar to taking PrEP) and you avoid it. As with COVID any breakthrough infections should be more mild.
-
I think there's a lot they don't know, but… https://www.nature.com/articles/d41586-022-01493-6
-
Well, New York City is now up over 1,000 cases (1,040 to be exact). The CDC (using slightly older state-level data) says just under 1/3rd of the US cases (31%) are in New York State. California only has about 40% of the cases we do despite having double the population.
-
Tell me what you think of my logic here… #Monkeypox IS an STI. It’s just not ONLY an STI. Important distinction there… It’s kinda like “all lives matter” (truly), but right now we need to talk about how black lives matter. Personally I think we do our community a disservice if we don’t get the word out that it’s being transmitted sexually, but the idiot anti-vax Republicans will then use that to stigmatize our community. Maybe telling them it’s like all lives matter / BLM will get them to understand. They don’t give a shit about BLM and that’s the equivalent of STI in this analogy, so they should focus on the all lives matter part (that it can be transmitted many other ways). Then again, “haters are gonna hate” no matter what you do, so…
-
Some localities are pushing back and defying the CDC/FDA on the 2nd dose. San Francisco has now said it will be putting off the 2nd dose… https://apple.news/AyW4eUNIETCyxAq3miLAJaQ I saw something somewhere that Colorado will only be giving first doses as well (for now). Refer to the Science.org article above for why this is OK (there's solid science behind just one dose for now). It's also what Canada is doing. Remember - it makes no difference to you if you get your 2nd dose 4 weeks later or 2 years later. The only way to get Mpox to go away quickly is to get lots of first doses rolled out. So please refuse your 2nd dose until everyone who wants one can get their first dose. In other Bay Area news… Monkeypox has been detected in the waste water of 10 of the 11 areas that are monitored. https://apple.news/AIiZPTIWwQoWGXSdhKocnZQ
-
Our community is somewhat legendary for working with health authorities on things like contact tracing. And the fact that thousands of vax appointments here in NYC are gone in 7 minutes says a lot about our community’s willingness to do stuff to end this. I refuse to blame the victim on this one. Read Peter Staley’s account of what the FDA and CDC have gotten wrong so far… https://apple.news/Am5peboTYQfuX_N0R_WS6QQ It’s appalling. It’s incompetent. They literally learned nothing from COVID. The 7 day average increase in cases in NYC was 9.5% PER DAY this past week. I’d bet money it was a lot lower in Montréal and Toronto where they have adequate vaccine supplies. That means it’s not us, it’s them. (Does anyone have the data for MTL or TO?) That said, could we do more? Absolutely. This weekend is Pines Party weekend. I’m mortified it wasn’t canceled. It will be a super spreader event. Rumor is they somehow have vaccines and are going to try to vaccinate everyone who shows up. But that’s only going to make the cases more mild - it won’t stop infections or spread. On the other hand fewer guys are showing up. The Pines is quieter than a normal Pines Party weekend, and I saw a comment about how the CumUnion party in MTL was pretty sparsely attended. So people are pulling back. Would it be wonderful to have a few weeks each year when people stop having sex and everyone gets tested? Yeah. But that’s not a realistic goal. You have to deal with reality.
-
Justice Thomas makes it clear decisions support our rights are next
rawTOP replied to drscorpio's topic in LGBT Politics
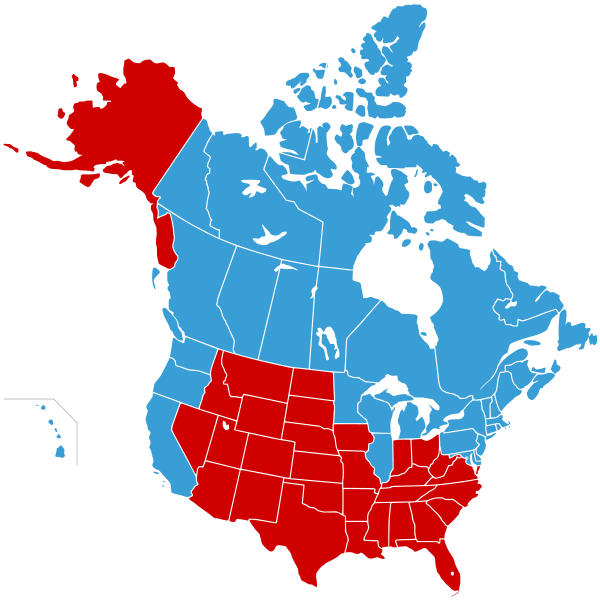
The solution I’ve seen is this… The United States of Canada and then Jesusland (ruled by the American Taliban)… I feel sorry for New Mexico they’re the blue oasis in Jesusland. Maybe they can join Mexico (but that’s not nearly as good as joining Canada). Personally I completely support a national divorce. For a long time now I thought the Civil War was a mistake. We should have just let them go their own way and taken in any slave that managed to get to the Union.
-
If none of them have puss, then almost certainly not Mpox.
-
Vaccines in Canada are mostly given out in the main gay centers - Montréal and Toronto, and to a lesser extent Vancouver. Your friends should look at the City health department websites for each of those places. Here’s an article on the situation in Canada… https://apple.news/ALH6Jf1AuSyuSLETxRHxODg
-
https://www.medscape.com/viewarticle/977532 ^^^ This ^^^ is why it's important to refuse your 2nd dose if you've already gotten your first. There's not enough to go around and it won't make any difference to you if you get your 2nd shot next year when they'll get the extra doses.
-
Actually even after it goes away it's still infectious until the skin regrows - which happens roughly a week later in most cases.
-
Progress on combatting drug-resistant STIs
rawTOP replied to rawTOP's topic in HIV/AIDS & Sexual Health Issues
And another article about how Chinese researchers have made progress as well, though along more traditional research lines… https://apple.news/AZMD6UHDKQwyqqYbi1NcFpg -
If you want a vaccine shot and can’t get one and have some money to burn or frequent flyer miles… Go to Canada. Toronto doesn’t require an appointment, ID or a health card - you just get in line and they give you a shot (It’s what I did - I happened to be there). Be prepared to give a Canadian address and phone number - though you could probably give the address of a hotel and a US phone number and they’d be fine. Montréal requires an appointment but I saw something on Twitter saying they will vaccinate tourists. It’s sad that folks in the US have to resort to this. But when it came to COVID the situation was reversed. I know NYC was giving shots to tourists and Canadians were coming here to get them. So it’s not like you have to be ashamed of using their health system when we let them use ours not so long ago. And again - if you’re in the US - please refuse your 2nd shot until all your gay brothers have had a chance to get their 1st shot. You can get your 2nd shot any time in the next 2 years and have the same level of protection.