fskn
-
Posts
812 -
Joined
-
Last visited
.thumb.jpg.d569cbbe53ee0f6995a4e7d2810ecb4d.jpg)








Recent Profile Visitors
27,885 profile views




fskn's Achievements
")





-
I want you to get me pergnet as soon as possible
-

Deal, oh I mean nice invite to pregnant you.
-
-
And here it is, folks, the concurring opinion of the longest-serving Supreme Court justice (who also happens to be African American, which is neither here nor there, but is interesting to note, in that race and progressiveness are totally unrelated): "The same rationale that the Supreme Court used to declare there was no right to abortion, [Clarence Thomas] said, should also be used to overturn cases establishing rights to contraception, same-sex consensual relations and same-sex marriage." Source: [think before following links] https://www.nytimes.com/2022/06/24/us/clarence-thomas-roe-griswold-lawrence-obergefell.html To understand why Thomas' opinion matters, it's important to realize that, even though Roberts still holds the title of Chief Justice, Thomas has the right to assign opinions. He is the senior member of the court's conservative majority. Source: [think before following links] https://edition.cnn.com/2021/07/21/opinions/clarence-thomas-supreme-court-power-toobin/index.html I actually like to be proved wrong in spirited, substantive debate. On this issue, I would have been relieved to be wrong. But the people who said there was nothing to worry about never offered any substantive evidence to support their position, and it is now clear that they were mistaken. Within a matter of years, your same-sex marriages will be invalidated, it will again be illegal for you to engage in gay sex, you won't be allowed to get condoms even if you want them (yes, this is a bareback enthusiast site and primarily one for people who are not physically able to have children, but the thought that access to contraceptives will once again be restricted is chilling), and who knows what other hard-won, long-fought-for rights and freedoms will be abrogated? Please, please exercise your right to vote in the 2022 midterm elections...
-
@BBBlondie, wow! 🤤😉 And may I add that I have the biggest admiration for people who are bold enough to post pics on public forums like this?
-
@TripA84, glad you've gone in for testing and treatment! Taking care of your sexual health shows that you care about yourself and about other people. Please consider discussing with your doctor, and setting up a regular testing schedule. Although people who take medication for HIV prevention or HIV treatment automatically receive regular STI testing (for PrEP users who are gay or trans, the US guideline is STI testing every 3 months), other people should consider regular testing, too. Unless we stop having sex, STI risk is always present. It's also a good idea to review vaccinations with your doctor. Vaccines against Hepatitis A, Hepatitis B, HPV, and meningitis are available, and these four infections can be transmitted sexually. As you and @hntnhole both say, these are the risks we take. Note too that gonorrhea and some other STIs can be transmitted just from getting or giving a blowjob. Reference re: testing frequency: • Search for "More frequent STI screening" in [think before following links] https://www.cdc.gov/std/treatment-guidelines/msm.htm
-
I like the idea of reminding people in general — or were you thinking of a flag that the person who starts a particular new thread can set, to indicate that bugchasing discussion isn't the purpose of the thread? (A field for "What this thread is not about" could benefit both those who dislike fetishes and those who like them. For example, every time someone brings up cheating sex, people with moral objections drown out erotic discussion, making it impossible to discuss cheating as a fetish. Separating the fetish angle of a subject from other angles, such as moral or medical angles, leaves everyone a space.)
-
@Omnivac, don't feel that you have to ask him to define the relationship. Although talking and asking questions can clarify a relationship, it's easy to forget that the other person might not be ready to answer on our timeline. Sometimes a person hasn't figured everything out yet. Even if there is an immediate and precise answer, we are constantly growing and changing, and a relationship is dynamic in and of itself. How he behaves matters more than any words he might say if you asked about his intentions toward you. I wouldn't worry about cheating, homewrecking, etc., either. Our behavior reflects what we truly want, and moving toward what we want, however difficult the process, is good for us. If he did pursue a romantic and/or sexual relationship with you, it would be for you to decide whether you were satisfied with the level of involvement he could offer, given his existing family. Eventually, it would be for him and his wife to decide the fate of their marriage, and for them to work through any issues with their children. (Those concerns would be in the future, and in any case, people are more resilient than we give them credit for.) It sounds as if you and this man have a special bond. Enjoy your time together, whatever the outcome!
-
 I do neither. I have pointed out from my first message that DoxyPEP is a research study, and that a recommendation, if ever there is one, would be in the future. I have always quoted study material, with its caveats. I use terms like "off-label" (which means not FDA-approved) frankly. In every message, I advocate discussing with a medical professional, never persuading one. You seem to go rather far in the opposite direction, speculating — though you are clearly not a participant in the study, and don't meet regularly with researchers in this field, as I do — that STI PEP will increase resistance. Professionals aren't sure, which is why they continue to conduct research, and why they decide, in clinical practice, whether the potential benefits of an off-label prescription outweigh the potential risks. My regular physician — licensed in California and not party to the study — has decided to provide me with doxycycline. The study researchers, the study's Data Safety and Monitoring Board, and institutional review boards (ethics watchdogs) at multiple levels have also decided to offer doxycycline to all study participants who had been randomized to the control/standard of care arm and did not originally receive it. You seem to think you know better than them, but, as I tell everyone, talk to and trust your licensed medical professional!
I do neither. I have pointed out from my first message that DoxyPEP is a research study, and that a recommendation, if ever there is one, would be in the future. I have always quoted study material, with its caveats. I use terms like "off-label" (which means not FDA-approved) frankly. In every message, I advocate discussing with a medical professional, never persuading one. You seem to go rather far in the opposite direction, speculating — though you are clearly not a participant in the study, and don't meet regularly with researchers in this field, as I do — that STI PEP will increase resistance. Professionals aren't sure, which is why they continue to conduct research, and why they decide, in clinical practice, whether the potential benefits of an off-label prescription outweigh the potential risks. My regular physician — licensed in California and not party to the study — has decided to provide me with doxycycline. The study researchers, the study's Data Safety and Monitoring Board, and institutional review boards (ethics watchdogs) at multiple levels have also decided to offer doxycycline to all study participants who had been randomized to the control/standard of care arm and did not originally receive it. You seem to think you know better than them, but, as I tell everyone, talk to and trust your licensed medical professional! -
Staring At Men's Dicks While In A Restroom?
fskn replied to BlowBoi's topic in Cocksucking Discussion
I hope you're the kind of guy who pulls his pants part-way down at a urinal, because I'd be looking at that ass...forget peeping over the partition, I'd be looking from behind you! 😉- 93 replies
-
- 5
-

-
-
- cocksucker
- gay
- (and 3 more)
-
Regarding DoxyPEP and fears about resistance, I defer to medical professionals. I know more than the average person, but much, much less than the researchers, clinicians and clinic leaders who are working on the DoxyPEP study, and on STI treatment in general. Ethics review boards at multiple levels are also involved. A few points to consider: • Doxycycline won't be handed out like candy. No responsible professional would prescribe it — off-label, at that — to a patient not at high risk of STIs. The people for whom this prevention strategy might make sense already have high STI rates. • Resistance is complex. If you worry that using small, episodic doses of doxycycline (an older antibiotic) to prevent STIs might increase the prevalence of antibiotic-resistant bacteria, why not also worry that failing to prevent STIs might increase resistance? More infected hosts; more time between infection, diagnosis, and treatment; and presumptive (and reasonable and recommended, but nevertheless presumptive) use of a wider range of old and new antibiotics for treatment, in larger doses and/or for more days at a time; might turn out to be worse across a high-risk population like men who have sex with men (MSM). • A great feature of the DoxyPEP study is resistance testing every time a participant gets a bacterial STI. Because there's a (legitimate) desire to treat people who have STI symptoms quickly, cheaply, and in a standardized way, resistance testing is not routine. Outside of studies, resistance testing happens after treatment failure, once it becomes necessary to try a different antibiotic. DoxyPEP participants who test positive for STIs get standard treatment, with no extra wait, but their test specimens are kept so that resistance testing can be done later, to look for patterns. If we took a less commercial, less short-term view of medical costs, we'd be doing resistance testing routinely on STI test specimens, to track resistance proactively rather than reactively. • Whether to use doxycycline for STI PEP is a discussion between patient and medical professional. The uniquely American, consumerist practice of medicine by TV commercial (where we're told to ask for novel prescription drugs by name) is unethical, expensive, and dangerous to our health. A conversation should start with "Would this make sense for me?" rather than "Prescribe this for me, because I saw an ad for it on Lifetime/read about it on Facebook!" I certainly don't think we should shop for doctors who will say yes. Rather, when we encounter a doctor who says no, we should make sure that the decision is not borne of prejudice, outdated knowledge, or lack of experience treating GLBT patients.
-
That is totally different. It's treatment rather than prevention, and one-time rather than routine. Self-treatment is risky because even if a person could be certain of having a particular infection, appropriate treatment for bacterial STIs is complex and ever-changing. The US guidelines for treating gonorrhea have changed within recent memory, for example. This is not to say that treatment strategies that give patients more control are bad, when used in cooperation with medical professionals. For example, US guidelines have long recommended "expedited partner therapy" (EPT). A patient can ask for extra doses of STI treatment medication to hand directly to sexual partners. That's a great way to reach people who do not have access to medical care or who simply would not go in for testing and treatment. A new California law specifically encourages partner treatment. US guidelines also recommend treatment for presumed infections, especially when available diagnostic tools are limited. The risk that a patient who has to wait days or weeks won't receive the test result, let alone return for treatment, is high. Once again, though, a medical professional is involved. Last but not least, the role of telemedicine is growing, but medical professionals must still arrange for patients to get tested, whether by going to a laboratory, by collecting specimens at home and mailing them in, by taking rapid self-tests under observation, or by taking rapid self-tests without online supervision. References: • See "Antimicrobial-Resistant N. gonorrhoeae" in [think before following links] https://www.cdc.gov/std/treatment-guidelines/gonorrhea-adults.htm • [think before following links] https://www.cdc.gov/std/treatment-guidelines/clinical-EPT.htm • [think before following links] https://sd06.senate.ca.gov/news/2021-10-05-governor-signs-sb-306-tackle-sti-crisis • Search for "presumptive" in [think before following links] https://www.cdc.gov/std/treatment-guidelines/urethritis-and-cervicitis.htm • See "Providing PrEP by Telehealth" on p. 40 of [think before following links] https://www.cdc.gov/hiv/pdf/risk/prep/cdc-hiv-prep-guidelines-2021.pdf
-
Do tops like sloppy well used cum dripping assholes?
fskn replied to Oralguya1's topic in General Discussion
I can tell, and I love it. Some tops seem to get jealous, but I'd just be proud of my bottom. Sharing is caring! It's more fun and, paradoxically, it can strengthen a relationship. The expectation of exclusive access to a bottom's hole gives way to, "Hmmm, I want you to get bred by other guys because fucking your sloppy hole feels even better for me." -
Staring At Men's Dicks While In A Restroom?
fskn replied to BlowBoi's topic in Cocksucking Discussion
Partitions between urinals ought to be banned. Maybe we should lobby building code committees. 😂 There's a beautiful building in my town with old-fashioned full-height porcelain urinals (the kind that are set into the wall and into a raised step). It would be very hard to add partitions, and impossible without damaging the historic fixtures, wall tiles and floor tiles. The restroom isn't busy so I've never seen anything there, but it makes me happy to know that such a place still exists. Ditto for trough urinals, of which so few remain. When did we become so ashamed of our bodies that we felt we needed partitions to be able to pee?- 93 replies
-
- 7
-
-
- cocksucker
- gay
- (and 3 more)
-
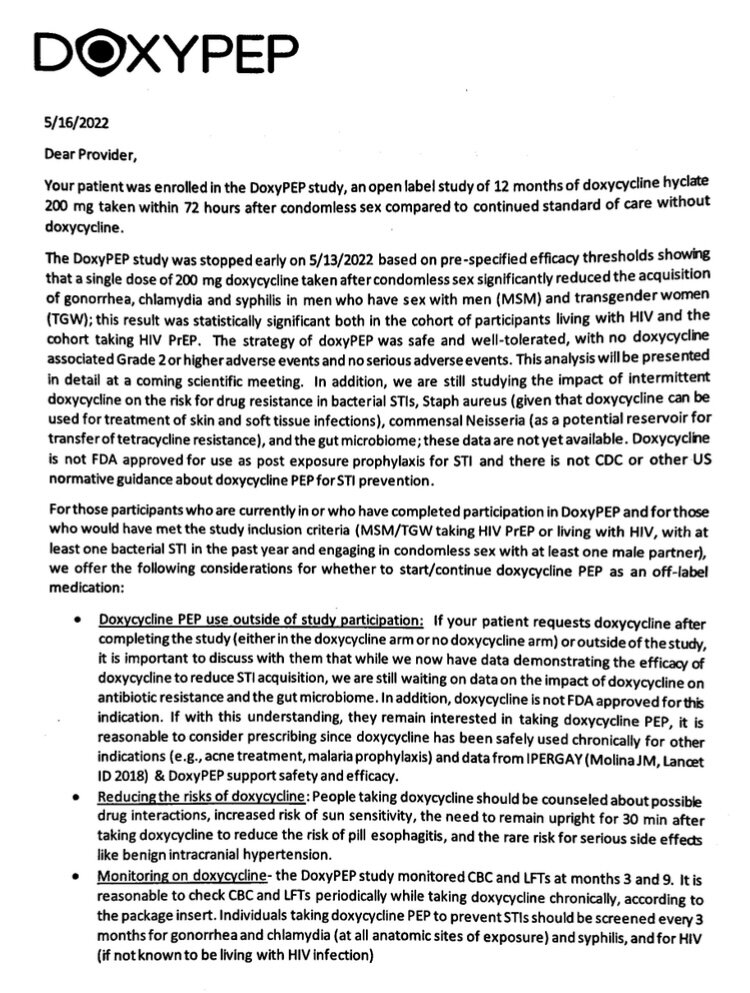
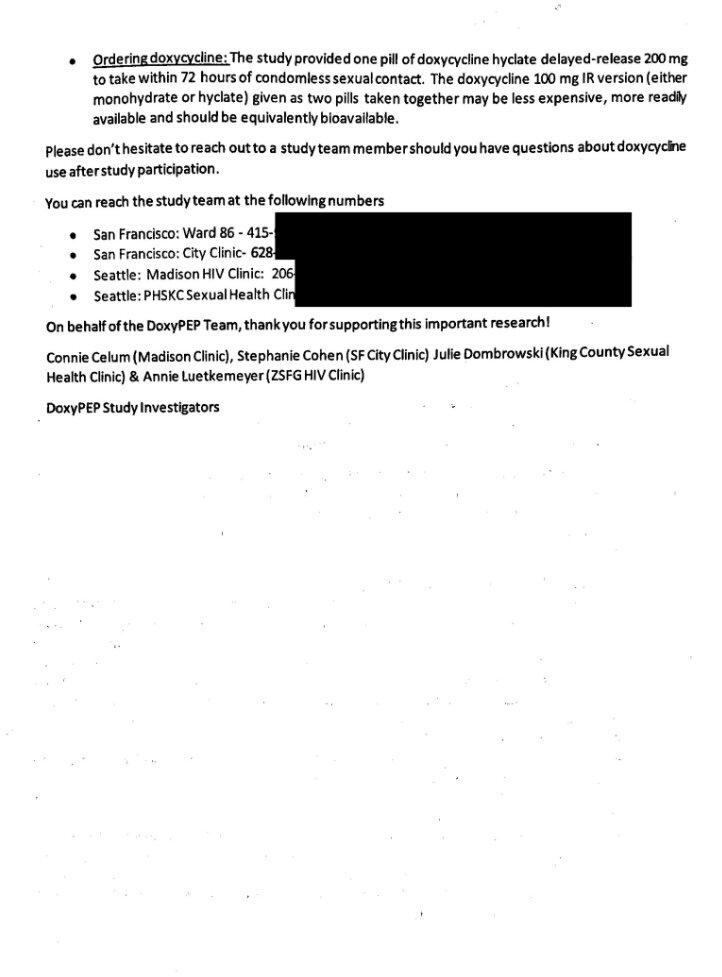
It would require a discussion with your doctor (or other professional licensed in your state to prescribe medications, perhaps a nurse practitioner or physician's assistant). Discussion is especially important because this would be an "off-label" use. If your medical provider is aware of gay (and trans) sexual behavior, is humble enough to seek new information, perhaps by contacting one of the DoxyPEP principal investigators, and is flexible, you might be able to move to a conversation about whether this approach is right for you. If you receive a flat-out refusal, see if you can find a doctor who has experience serving GLBT patients, or go to a community clinic with that focus. Here is the "provider letter" being given to study participants, for us to pass on to our regular doctors. My doctor was happy to prescribe doxycycline. I'd love to hear, via this thread, from other people who have asked for and/or received doxycycline for STI PEP. The evidence of efficacy from the DoxyPEP study was so strong that the experiment ended early, and participants not assigned to receive doxycycline will have the option. Separately, because doxycycline has been available for so many decades and is so widely used, there is plenty of evidence about its safety, side effects, and risks. There is also lots of evidence about the risks of antibiotics generally. (The DoxyPEP researchers are continuing to monitor study participants, to look for any antibiotic resistance patterns.) A recommendation to use doxycycline for STI PEP would take a long time and a label change, even longer — if either outcome ever happens. This doesn't mean access should be or will be impossible. For example, intermittent or "2-1-1" Truvada for HIV PrEP is supported by research and has been added to the CDC PrEP guidelines, even though the product hasn't been relabeled. When Truvada for PrEP is prescribed with less than daily dosing, that's an evidence-based but nevertheless off-label use. Good luck!